The Aging Heart: Understanding Cardiovascular Changes After 60
The heart stiffens, arteries lose elasticity, and VO2 max declines. But with the right exercise prescription, these changes can be significantly slowed. Here's what every senior healthcare specialist needs to know.
The cardiovascular system undergoes profound structural and functional changes with age — changes that are often mistaken for disease but are in fact normal physiology. Understanding these changes is essential for any senior healthcare specialist designing safe and effective exercise programs.
Structural Changes in the Aging Heart
The heart muscle itself undergoes several changes after 60. The left ventricular wall thickens (hypertrophy) as the heart works harder against stiffer arteries. The heart muscle becomes less compliant — it does not relax as quickly between beats, which impairs the filling of the ventricles (diastolic dysfunction). This is why many elderly patients develop heart failure with preserved ejection fraction (HFpEF) — the heart pumps adequately but cannot fill properly.
The cardiac conduction system also changes. The sinoatrial node (the heart's natural pacemaker) loses cells with age, reducing the maximum heart rate achievable. The classic formula for maximum heart rate (220 minus age) reflects this biological reality.
Arterial Stiffening: The Central Problem
The aorta and large arteries lose elasticity with age as collagen accumulates and elastin degrades. Stiff arteries cannot buffer the pulse pressure generated by each heartbeat, leading to higher systolic blood pressure and lower diastolic pressure — the characteristic wide pulse pressure of elderly hypertension.
Arterial stiffness is not just a consequence of aging — it is a driver of further cardiovascular damage. The reflected pressure wave from stiff arteries arrives earlier in the cardiac cycle, increasing the workload on the left ventricle and accelerating its stiffening.
VO2 Max Decline: The Fitness Cliff
VO2 max — the maximum rate of oxygen consumption during exercise — declines at approximately 10% per decade after age 25 in sedentary individuals. By age 70, a sedentary person may have lost 40–50% of their peak aerobic capacity.
This decline has profound functional consequences. Activities of daily living — climbing stairs, carrying groceries, walking to the market — require a fixed absolute oxygen consumption. As VO2 max falls, these activities represent an ever-larger percentage of maximum capacity, becoming progressively more exhausting.
The Good News: Exercise Attenuates These Changes
The cardiovascular changes of aging are real, but they are not inevitable in their severity. Regular aerobic exercise significantly attenuates the decline in VO2 max, reduces arterial stiffness, and improves diastolic function. Studies of master athletes show cardiovascular function decades younger than their sedentary peers.
For elderly patients, the exercise prescription must account for the reduced maximum heart rate and the longer recovery time needed between sessions. PHA coaches are trained to use rate of perceived exertion (RPE) alongside heart rate monitoring to ensure appropriate exercise intensity.
Practical Implications for Praan Health Coaches
When designing cardiovascular exercise programs for elderly clients, PHA coaches consider: the patient's baseline functional capacity (assessed with the 6-minute walk test or step test), the presence of cardiac medications (beta-blockers reduce maximum heart rate), the importance of adequate warm-up and cool-down (the aging heart takes longer to adjust to changes in demand), and the value of interval training (alternating moderate and light intensity) over continuous high-intensity exercise.
The goal is not to push the aging heart to its limits — it is to systematically expand those limits over time, restoring functional capacity and quality of life.
References & Further Reading
- [1]Lakatta EG, Levy D. Arterial and cardiac aging: major shareholders in cardiovascular disease enterprises. Circulation. 2003;107(1):139-46.
- [2]Fleg JL et al. Accelerated longitudinal decline of aerobic capacity in healthy older adults. Circulation. 2005;112(5):674-82.
Category
Learn This in 21 Days
Everything in this article is taught in depth during the PHA certification program.
Enroll Free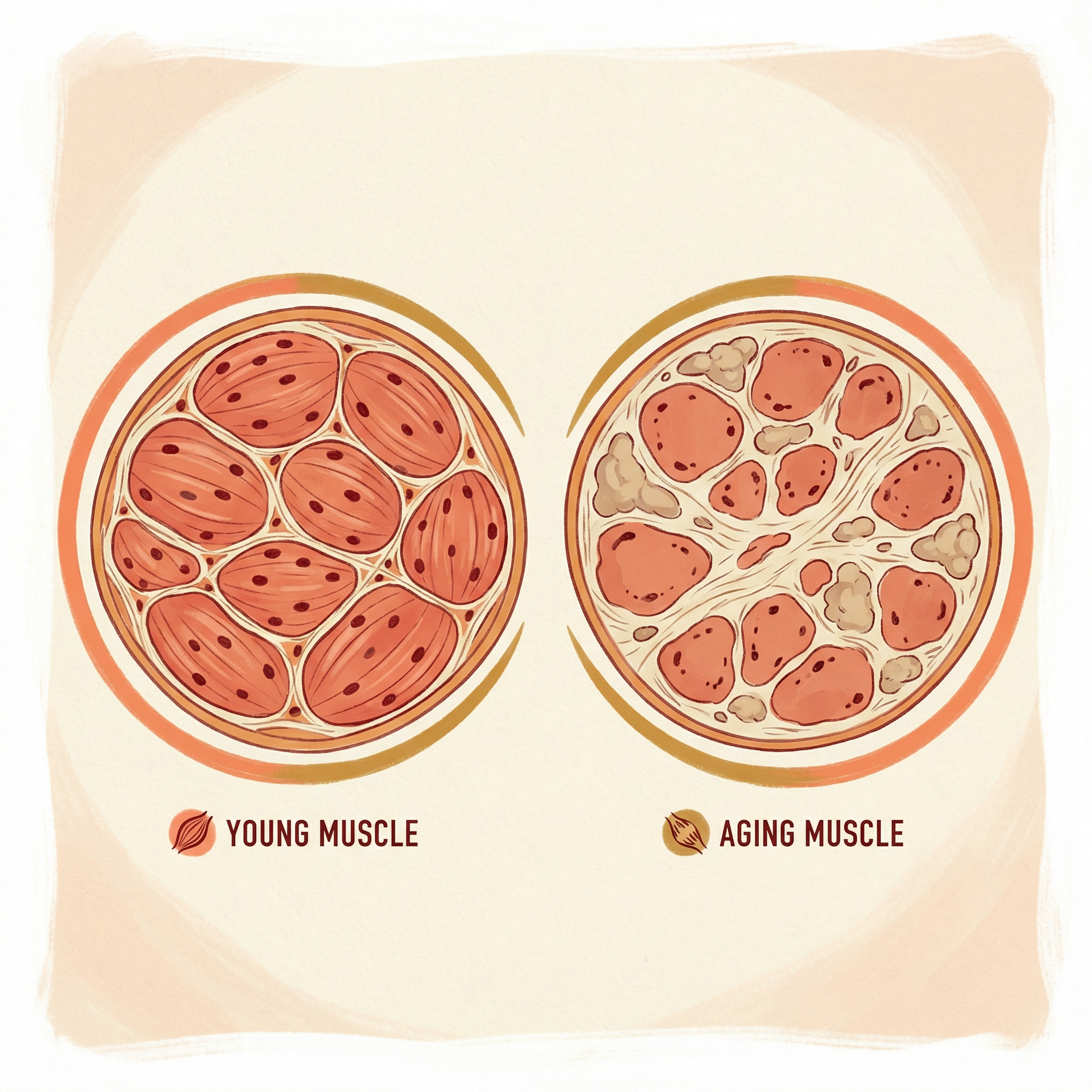
Ready to Apply This Knowledge?
The PHA 21-day certification teaches you to apply evidence-based senior healthcare with real patients.